How Do You Diagnose Conn's Syndrome of the Adrenal Gland?
There are a number of tests that will help establish the diagnosis of Conn's Syndrome, but primarily we want to know if there is too much aldosterone being produced by one of adrenal glands since over production of aldosterone is the cause of this disease. The diagnosis of primary hyperaldosteronism (Conn's Syndrome) follows a logic three step approach that is:- Screening for the disease. This is done primarily with blood tests looking for excess aldosterone levels, high blood pressure (usually diastolic hypertension) and blood potassium levels (low to normal).
- Confirming the disease. These tests are repeated and a CT scan of the adrenal glands is performed.
- Performing subtype diagnosis.
Lab Testing for the Diagnosis of Primary Hyperaldosteronism (Conn's Syndrome)
The ARR Screening Test. The aldosterone to renin ratio (ARR) is the most reliable screening test for primary hyperaldosteronism. This is very easy to do and only requires one tube of blood to be drawn from your arm. Ask your doctor to get a simple blood test to check your plasma aldosterone concentration (PAC) and plasma renin activity (PRA). Classically, patients with primary hyperaldosteronism have: Plasma aldosterone concentration (PAC) = HIGH, and Plasma renin activity (PRA) = LOWIf dividing the PAC by the PRA: PAC/PRA (this is called ARR; aldosterone-renin ratio). If the result is greater than 20, then the patient is very likely to have primary hyperaldosteronism. typically, these patients will also have a low blood potassium level (hypokalemia), but in reality, less than half of patients have low potassium--most have low normal levels of potassium in the blood. a blood potassium level is a common blood test performed as part of a routine annual physical exam. Ask your doctor to go back and see if your potassium level has ever been low. Of course, if you must take extra potassium supplements then you are hypokalemic (you have low blood potassium). Remember, only a third or so of patients with primary hyperaldosteronism have low blood potassium levels, but if you do there is a strong likelihood that you have primary hyperaldosteronism since there is really no other reason to have low potassium (except for some drugs, like lasix and other diuretics).
Blood pressure medications that can interfere with testing for Conn's Syndrome and hyper-aldosteronism.- Spironolactone (Aldactone)
- Eplerenone (Inspra)
- Amiloride
- Beta-blockers (Metoprolol, etc)
- Clonidine
- ACE inhibitors (Lisinopril, Captopril, etc)
- Calcium channel blockers (Amlodipine, Diltiazem, etc)
- Diuretics (Lasix, etc)
Thus, if you are getting your blood tested for aldosterone and renin, it is in your best interest to not be taking any of these drugs. But, it is better to just test PAC and renin while on BP medications, than never having your levels checked at all. Obviously, you can't stop taking any of these medications without talking specifically about it with your doctor. Almost all of these drugs will make the blood test for Conn's Syndrome error in the direction of saying that you do NOT have it when you do--they don't error in the direction of saying you DO have it when you really don't.
Should Blood Pressure Drugs be Stopped Prior to Testing for Aldosterone-Secreting Tumors (Conn's Syndrome)?
Antihypertensive medications other than diuretics, should always be withdrawn for at least 4 weeks (6–8 weeks for spironolactone) before testing for an aldosterone secreting adrenal tumor causing Conn's Syndrome. Important! As discussed above, in many patients, this is not feasible because the blood pressure will go too high.The most important medications to stay off during testing are Spironolactone (Aldactone), Eplerenone (Inspra), Amiloride. If your doctor says it is not safe for you to stop your blood pressure medications for a few weeks, it is still better to have your testing done while on medications than not be screened at all.
Testing in the morning. The ARR test is most sensitive and most accurate when samples are collected in the morning after patients have been out of bed for at least 2 hours, usually after they have been seated for 5–15 minutes. Given that the screening test can be affected by medications, it may have to be repeated once (a couple of weeks apart).
However, for most doctors diagnosing primary hyperaldosteronism is hard, time-consuming and sometimes confusing (the exception being only a few medical endocrinologists who are focused on endocrine hypertension and some kidney doctors; medical nephrologists with a focus on secondary hypertension). If you or your doctor want to run the laboratory tests by us, please do! We are here to help. Send us your laboratory results including what medications you were on during the testing.
In addition to evaluation the ARR screening test, it is important to review the absolute aldosterone value (a plasma aldosterone concentration; PAC >15 ng/dl is highly indicative of the disease). Also, the lowest detectable level of plasma renin activity (PRA) should also be considered. A very low renin (That is, suppressed) almost always proves primary hyperalddosteronism. Importantly, laboratories need to report individual values for both plasma aldosterone concentration (PAC), and plasma renin activity (PRA), as well as the ARR.
Classic Cases of Hyper-Aldosteronism and Conn's Syndrome
Are you an "ALDO slam dunk"? Do you have classice hyperaldosteronism? So, to make things easier, let us start out with a text-book, classic patient with primary hyperaldosteronism. Are you an ALDO slam dunk? As you have read so far, arriving at the accurate diagnosis of primary hyperaldosteronism can be a bit tricky. However, this is easy for us. We evaluate patients with potential primary hyperaldosteronism EVERY DAY! Text-book cases are what we call ALDO slam dunks. These are patients it is so obvious that they have primary hyperaldosteronism, a third-year medical student should be able to pick it up. About 80 % of our patients with primary hyperaldosteronism are ALDO slam dunks. These are some of the characteristics of an ALDO slam dunk.The Classic Patient with Hyper-Aldosteronism (Conn's Syndrome). The "ALDO Slam Dunk"
- High blood pressure (relative short duration)
- Tend to be female
- Young age (< 50 years old)
- Low blood potassium (hypokalemia)
- No other risk factors for high blood pressure (smoking, obesity, kidney disease, diabetes, etc)
- Very high plasma aldosterone concentration (PAC); >15 ng/dl
- Low (suppressed) plasma renin activity (PRA)
- Hypertension responding well to Spironolactone (or similar drugs)
- May have symptoms (frequent urination, muscle cramps, fatigue, etc.)
If you are an ALDO slam dunk, in a way, congratulations. (Note, we do not take it lightly that you have a disease, but this is fixable!). You do not need to undergo any more confirmatory testing. You can move 2 steps ahead straight to an adrenal-protocol CT scan (if you cannot tolerate intravenous contrast, you can have an adrenal-protocol MRI). You may not need to have the adrenal vein sampling, but rather move 2 additional steps ahead straight to what will likely be a curative adrenalectomy. Read about curative surgery, Mini Back Scope Scope Adrenalectomy (MBSA)
All patients who are diagnosed accurately with unilateral primary hyperaldosteronism benefit from surgery, but women, and young patients tend to benefit the most. About 80 % of our patients with primary hyperaldosteronism are ALDO slam dunks. Yes, the operation will prevent you from developing future strokes, heart attacks, and arrhythmias (for instance, atrial fibrillation), and premature death.
Dr. Carling, Editorial note: For our international patients, the measurements of plasma aldosterone concentration (PAC) and plasma renin activity (PRA) are typically expressed in conventional or SI (Systeme International) units, meaning pmol/l (not ng/dl), and pmol/l/min (not ng/ml/h), respectively. Do not worry about this. Dr. Carling is used to evaluating laboratory data from around the world and can easily make sense of this. It is helpful, though, to include the reference range of any assay from the laboratory when you send us your data.
Confirmatory Tests for Hyperaldosteronism and Conn's Syndrome
Some patients are not an ALDO slam dunk and, thus, will need further testing. About 80 % of our patients with primary hyperaldosteronism are ALDO slam dunks, but that means about 20 % of patients need more detailed work up. This is where the confirmatory tests come in.The first confirmatory test you should have done is to repeat the aldosterone to renin ratio (ARR) as it is the most reliable screening test for primary hyperaldosteronism. Again, screening is easy. Ask our doctor via a simple blood test to check your plasma aldosterone concentration (PAC) and plasma renin activity (PRA).
Borderline Cases... Not Quite Sure? The Endocrine Society (based out of the United States) guidelines recommend that patients with borderline (equivocal) ARR, and plasma aldosterone concentration (PAC) should undergo a confirmatory test to definitively confirm or exclude the diagnosis of primary hyperaldosteronism. One of the issues are that the medical endocrinology and medical nephrology experts have had difficulties in identifying what is the ideal confirmatory test. The Carling Adrenal Center recommends that you have a 24-hour urine collection of your aldosterone level. If this level is in the high upper normal range or frankly elevated, this proves that you have primary hyperaldosteronism.
However, the following (somewhat cumbersome) test have been advocated by some. These tests are very rarely needed these days and most doctors would not use these outdated tests:
- Oral sodium loading test
- Intravenous saline loading test
- Fludrocortisone suppression test
- Captopril challenge test
Its Time To Get A Scan!
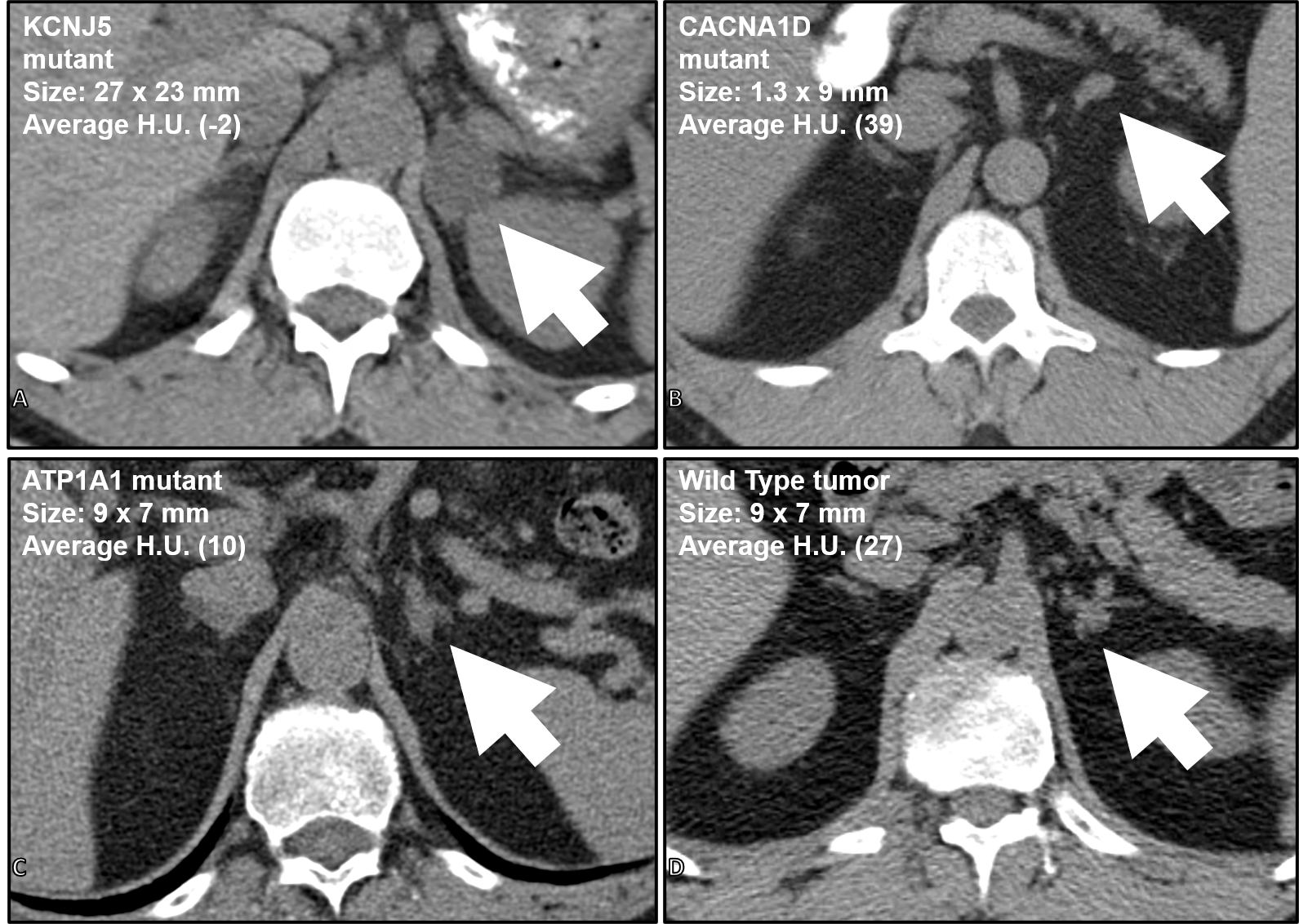 CT scans from 4 different patients all with a left aldosterone-producing tumor (arrows) causing primary hyperaldosteronism. Based on the characteristics of the genetic alteration, patient, and CT scan characteristics, predictions can be made whether the patient can go straight to surgery or need adrenal vein sampling.
Once the confirmatory test proved that the diagnosis of primary hyperaldosteronism is accurate you may move ahead to the next step: adrenal imaging with an adrenal-protocol CT scan (if you cannot tolerate intravenous contrast, you can have an adrenal-protocol MRI). We have an entire section of this large website on scans and x-rays for adrenal tumors. Bottom line, there really is ONE first scan to get: a CT scan (CAT scan) with contrast. 90% of people with adrenal tumors need only ONE scan! Read about adrenal X-rays and scans.
CT scans from 4 different patients all with a left aldosterone-producing tumor (arrows) causing primary hyperaldosteronism. Based on the characteristics of the genetic alteration, patient, and CT scan characteristics, predictions can be made whether the patient can go straight to surgery or need adrenal vein sampling.
Once the confirmatory test proved that the diagnosis of primary hyperaldosteronism is accurate you may move ahead to the next step: adrenal imaging with an adrenal-protocol CT scan (if you cannot tolerate intravenous contrast, you can have an adrenal-protocol MRI). We have an entire section of this large website on scans and x-rays for adrenal tumors. Bottom line, there really is ONE first scan to get: a CT scan (CAT scan) with contrast. 90% of people with adrenal tumors need only ONE scan! Read about adrenal X-rays and scans.
In many cases, Dr. Carling can predict where the excess aldosterone is coming from based on the CT scan. In fact, he has published extensively about this topic. Based on a combination of laboratory studies, the patient characteristics, genetic changes occuring in an aldosteronoma, and the findings on a CT scan, he can predict which patients can go straight to surgery versus the ones that will need more studies (i.e. adrenal vein sampling).
What is Adrenal Vein Sampling and Do I Need It?
Maybe, but many patients do not. Adrenal vein sampling (AVS) is sometimes needed to distinguish unilateral from bilateral adrenal sources of aldosterone secretion. This is an interventional radiology study. AVS should be performed in all patients with a CT scan that is questionaable or demonstrates adrenal tumors on both the right and the left side. Through small catheters blood samples are obtained from each adrenal vein and the inferior vena cava sequentially, or simultaneously. In experienced centers, the bilateral adrenal veins are catheterized and sampled with a technical success rate exceeding 90%. Technical success is directly associated with operator experience. You need the best radiologist to do this study! Most interventional radiologists do not perform it frequently. Ask your endocrinologist and radiologist how many of these studies they perform per year. Less than 10/year is not good enough.What are the top 10 Things to Know About Adrenal Vein Sampling for Primary Hyperaldosteronism (Conn's Syndrome)? Read more on our adrenal surgery blog
Dr. Carling, Editorial note: Unless your endocrinologist has extensive experience in identifying the best interventional radiologist to perform the Adrenal Vein Sampling procedure (if you need it), call us! We know who can do this procedure with great success rates and safely. But remember, MOST patients with Conn's Syndrome and hyperaldosteronism do not need Adrenal Vein Sampling. The advantage of AVS is that it proves whether the tumor comes from just one adrenal, and whether it is from the right or the left side.
Again, if you have primary hyperaldosteronism, let us review your imaging (send us your CT scan). Dr. Carling has more experience looking at adrenal tumors on CT scans (and has published widely about it) than almost any endocrinologist or radiologist (X-ray) doctor in the world. Also, do not waste time obtaining unnecessary expensive scans (for instance an MRI that almost nobody with this type of adrenal problem needs), or an invasive adrenal vein sampling procedure. Rarely you may need it, but most often you don’t. Dr. Carling has seen it all. He has created the scientific basis of the disease via the major international studies and can in minutes figure out provided what is going on with your aldosterone-producing adenomas (APA).