What is the Risk of Cancer in an Adrenal Gland Tumor or Adrenal Mass?
"Is it cancer?" is a very common question we hear at the Carling Adrenal Center. It is important to know that adrenal cancer is quite rare and over 95% of adrenal masses and growths are benign. Thus, risk that you have adrenal cancer is very low based on simple statistics. Adrenocortical cancer and malignant pheochromocytomas are very uncommon. On the other hand, benign adrenal tumors (which may or may not overproduce hormones) are quite common.The size of the adrenal mass is a very important characteristic to determine if it is cancer. The size of the tumor is very important in order to figure out whether it is cancerous or potentially cancerous. Very small tumors measuring 1 to 2 cm (less than an inch) are almost never cancerous. However, the larger the tumor is, the more likely it will be an adrenal cancer.
Should Small Adrenal Tumors be Removed?
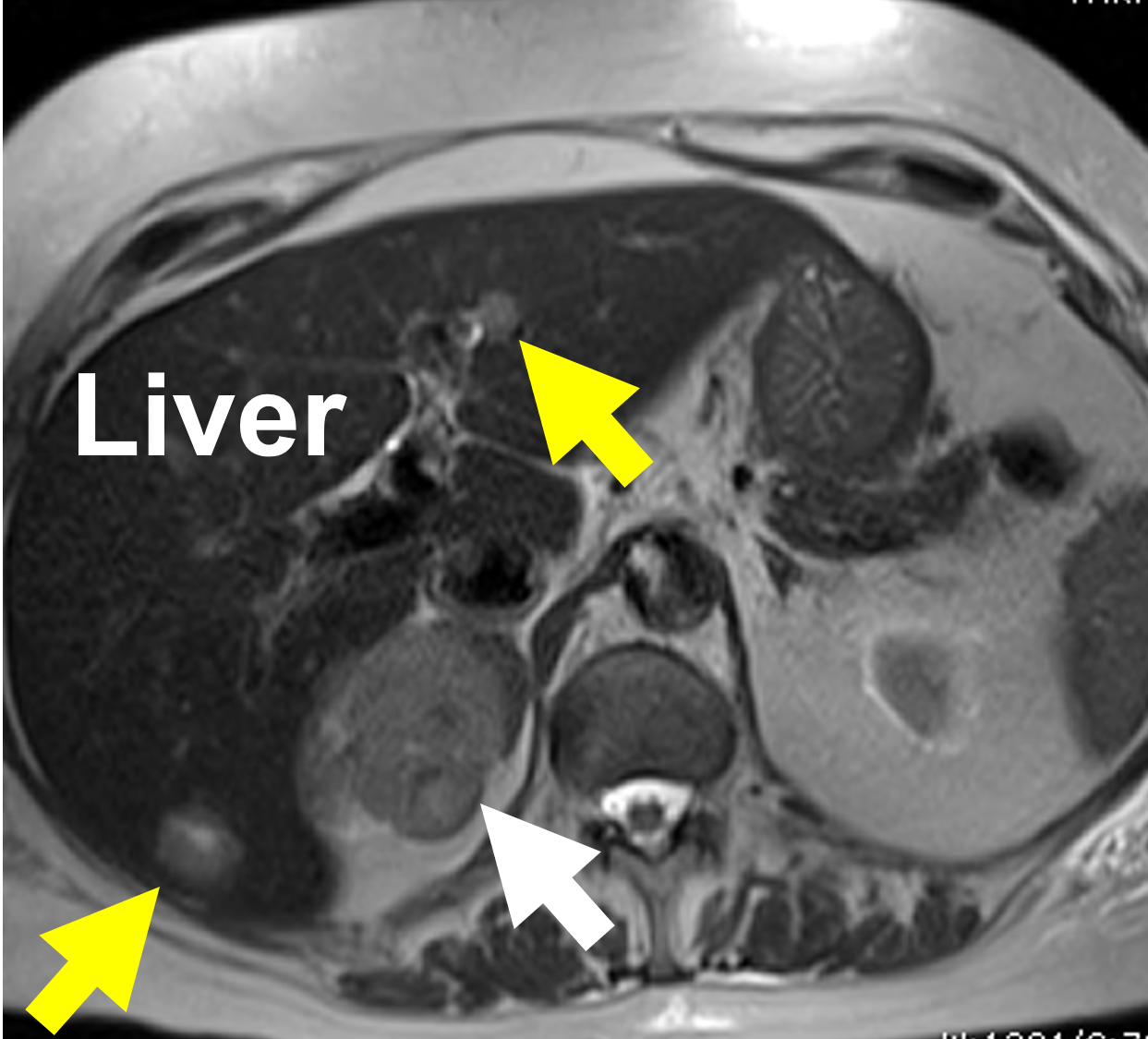 A larger tumor is more likely to be a cancer. This MRI displays an 8 cm right adrenal cancer (white arrow). This patient already had spread (metastasis) to the liver (yellow arrows) at the time of diagnosis.
We recommend removing any adrenal tumor or adrenal growth that is 4 cm (1.5 inch) or above for almost all adults. For younger patients, we would use a 3 cm (1.25-inch) cutoff. If you have a tumor that is 3 to 4 cm or larger, surgery is very likely your best option. This is a general guide and there are many exceptions to this rule. This is why you need to see a doctor--especially a surgeon--who has seen thousands of these cases and is an expert.
A larger tumor is more likely to be a cancer. This MRI displays an 8 cm right adrenal cancer (white arrow). This patient already had spread (metastasis) to the liver (yellow arrows) at the time of diagnosis.
We recommend removing any adrenal tumor or adrenal growth that is 4 cm (1.5 inch) or above for almost all adults. For younger patients, we would use a 3 cm (1.25-inch) cutoff. If you have a tumor that is 3 to 4 cm or larger, surgery is very likely your best option. This is a general guide and there are many exceptions to this rule. This is why you need to see a doctor--especially a surgeon--who has seen thousands of these cases and is an expert.
What Can X-Rays and Scans Tell About Adrenal Tumor Being Cancer?
Size is not only the criteria in determining whether the tumor is potentially benign or malignant. When we look at the imaging (scans and x-rays) of the adrenal gland, whether it is a CT, MRI, PET scan or other imaging study, we need to have a whole-person approach and evaluate all aspects of the tumor and the patient. We carefully analyze the "imaging phenotype" of the tumor. The imaging phenotype describes all aspects of what the tumor looks like on your scan and helps us determine the likelihood of cancer. It should be noted, this is far from a perfect science and is very dependent upon the experience of your surgeon. In many cases we can never know for sure whether the tumor is cancerous unless we remove it via adrenalectomy.What we look for on an scans and x-rays is a combination of more than a dozen criteria giving us a total impression, called the "imaging phenotype". For instance, we carefully examine the size and the shape of the tumor. That means we will look at whether the borders are smooth or irregular, and whether the margins are clear or unclear. On a CT scan without contrast, it is important to look at the level of attenuation. Essentially, this is a measure of how dense (or fat-containing) the tumor is based on measurements of what is called Hounsfield Units (HU). The lower the Hounsfield Units (lipid-rich; i.e. fatty) are the more likely it is that the tumor is not a cancer, but rather the more common adrenocortical adenoma.
A high-quality CT scan using contrast is the most important x-ray or scan. All adrenal masses need to be evaluated on a CT scan using an "adrenal protocol", which means the scan is done with and without contrast. This can tell us how much blood is going into the mass and whether the tumor is vascular since typically benign adenomas are not vascular, whereas more vascular tumors tend to be either a pheochromocytomas or a malignant tumor.
MRI scans are almost never needed for adrenal tumors. So if your doctor orders an MRI scan (especially if he/she orders it before the CT scan), then you can be assured they are not an expert in adrenal tumors. MRI scans don't have a big role in adrenal surgery or the workup of adrenal tumors. If you do have one, however, the more intense (vascular) tumors are more likely to be either a cancer or pheochromocytoma.
Other things we look at on the CT Scan. We also look to see if there are any areas of the tumor that are dead or necrotic. We look for previous or present bleeding (hemorrhage) into the tumor mass, and we look for calcifications (calcium deposits). The growth rate of the tumor is also very important, so we want to know if the patient has had previous imaging scans of the adrenal glands. Faster growing tumors are usually cancerous. Remember that we want to review all your images. Yes, even if you had a scan for unrelated reasons 10 years ago, we want to review it to see what your adrenal glands looked like then.
Should the Adrenal Tumor or Adrenal Mass be Biopsied?
NO! A biopsy of the adrenal tumor is almost never helpful and most of the time it can cause significant problems! Important rule: DO NOT PERFORM A BIOPSY OF AN ADRENAL MASS. In fact, it can be very dangerous if the patient has a pheochromocytoma. The biopsy may produce an adrenergic crisis (read about adrenergic crisis in the pheochromocytoma and paraganglioma section of this site). If the patient has an adrenocortical carcinoma (adrenal cancer), the biopsy may spill tumor cells into the surrrounding tissues. The tumor cells can then implant in these nearby tissues and cause local recurrence. Thus sticking needles into an adrenal tumor can decrease the chance of curing the patient, so do not do it. Also, a fine needle biopsy can never distinguish between a benign and malignant adrenocortical tumor, and is thus a wasteful and meaningless, invasive procedure. If your doctor wants to biopsy your adrenal tumor, then please give us a call--you need to seek better advice. The only time to consider a biopsy of an adrenal tumor is if the patient has another cancer, typically of the lung, kidney, breast, colorectal or melanoma and one is suspecting an adrenal metastasis.Because we see this mistake made at least a few times a week, we will say it again: If you doctor sends you for a fine needle biopsy of the adrenal tumor, you need to tell them to read this! DO NOT PERFORM A BIOPSY OF AN ADRENAL MASS.
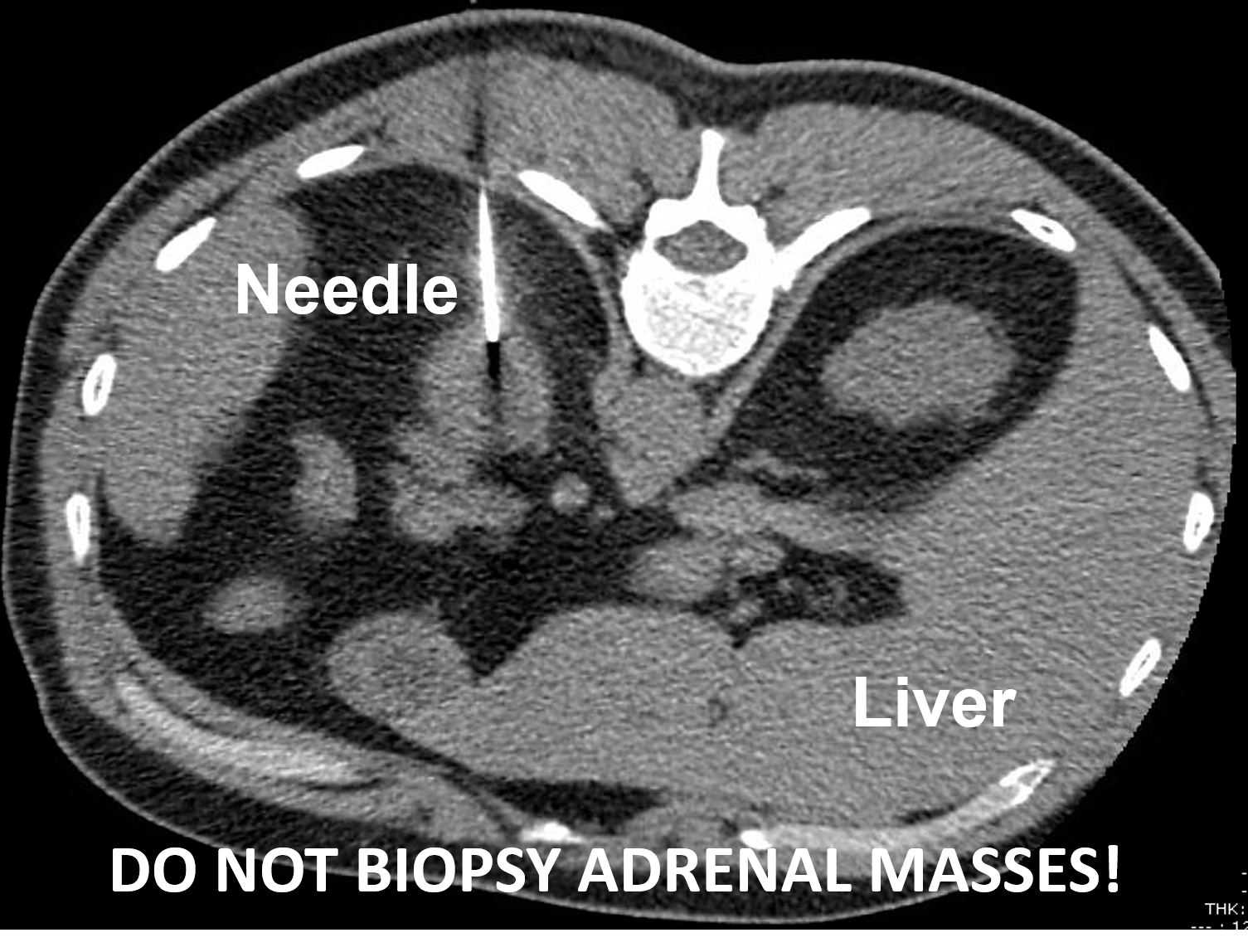 A left adrenocortical cancer undergoing a CT-guided biopsy. This should not be performed. The only time to consider a biopsy of an adrenal tumor is if the patient has another cancer and an adrenal metastasis is suspected.
The rule is to never biopsy an adrenal tumor. As with all rules, though, there are some rare exceptions. The only time to consider a biopsy of an adrenal tumor is if the patient has another cancer, typically of the lung, kidney, breast, colorectal or melanoma and one is suspecting an adrenal metastasis. Now you understand why patients with adrenal tumors should be seen by expert surgeons who have extensive experience with adrenal tumors. It can be somewhat tricky to know in advance of surgery whether the adrenal mass is cancerous, or not. Fortunately, the vast majority of adrenal tumors turn out to be benign. It is important to understand that sometimes surgery (adrenalectomy) is indicated just to prove that the adrenal tumor is not cancerous.
A left adrenocortical cancer undergoing a CT-guided biopsy. This should not be performed. The only time to consider a biopsy of an adrenal tumor is if the patient has another cancer and an adrenal metastasis is suspected.
The rule is to never biopsy an adrenal tumor. As with all rules, though, there are some rare exceptions. The only time to consider a biopsy of an adrenal tumor is if the patient has another cancer, typically of the lung, kidney, breast, colorectal or melanoma and one is suspecting an adrenal metastasis. Now you understand why patients with adrenal tumors should be seen by expert surgeons who have extensive experience with adrenal tumors. It can be somewhat tricky to know in advance of surgery whether the adrenal mass is cancerous, or not. Fortunately, the vast majority of adrenal tumors turn out to be benign. It is important to understand that sometimes surgery (adrenalectomy) is indicated just to prove that the adrenal tumor is not cancerous.
Read about the Mini-Back Scope Adrenalectomy (MBSA), which is the preferred operation for about 95% of people who need adrenal surgery.
It is important to understand that sometimes surgery to remove an adrenal mass (adrenalectomy) is indicated just to prove that the adrenal tumor is not cancerous. Said differently, sometimes we just don't know if an adrenal mass is a cancer until we get it out. If you have an expert adrenal surgeon, it is MUCH better to get the mass removed than to leave it in. Dr Carling does more adrenal operations than any other surgeon and he is happy to chat with you and your doctor about your adrenal mass.