Low Renin Levels, High Blood Pressure and Adrenal Tumors: 6 Things Every Hypertensive Patient Needs to Know

Here are a few key truths:
- All patients with high blood pressure should have their renin levels
- A low renin level almost always proves you have primary hyperaldosteronism (Conn syndrome).
- Primary hyperaldosteronism and the high blood pressure can often be cured with a 20–30-minute adrenal operation.
Yes, you read that right. A low renin almost always means you have primary hyperaldosteronism. It is so much more important to evaluate your renin levels than the aldosterone level (although both are important). The aldosterone level is often normal (yes, in the textbooks it is high, and your doctor may think it has to be high, but in real life, most patients have aldosterone levels in the normal range), so you have to look at them together (renin and aldosterone has to be evaluated together!). This is what we call the ARR (aldosterone renin ratio). An ARR above 20 suggests primary hyperaldosteronism. There are some exceedingly rare exceptions when the renin levels also are low such as the genetic disease Liddle syndrome, but in those cases, the aldosterone levels are low too.
So again, low renin level = primary hyperaldosteronism (in 99 % of cases)
Low Renin Levels, High Blood Pressure and Adrenal Tumors: 6 Things Every Hypertensive Patient Needs to Know
Hypertension, or high blood pressure, is one of the most common conditions worldwide, affecting nearly one-third of adults. While most cases are primary or essential hypertension, meaning there's no obvious cause, there are instances where hypertension stems from underlying diseases. The most common such condition is primary hyperaldosteronism (Conn syndrome), a form of secondary hypertension that is often undiagnosed, despite its potential to cause significant harm. In this article, we will explore how low renin levels, high blood pressure, and adrenal tumors are linked, and why diagnosing Conn syndrome is crucial for hypertensive patients.

Figure 1. If you have high blood pressure have your doctor check BOTH your renin and aldosterone levels.
What is Primary Hyperaldosteronism (Conn Syndrome)?
Primary hyperaldosteronism (PA), also known as Conn syndrome, is a condition where the adrenal glands produce excessive aldosterone, a hormone responsible for regulating sodium and potassium levels and maintaining blood pressure. Aldosterone helps control the balance of fluids in the body, prompting the kidneys to retain sodium and excrete potassium. When aldosterone production is uncontrolled, sodium retention increases, leading to water retention and high blood pressure (hypertension). In addition, potassium loss may result in hypokalemia (low potassium levels). Aldosterone secretion is normally controlled by the renin-angiotensin system (RAS), which helps regulate blood pressure and fluid balance. However, in Conn syndrome, aldosterone secretion occurs independently of this system, often due to adrenal tumors or hyperplasia of the adrenal glands.
Low Renin and High Blood Pressure: The Key Link
In primary hyperaldosteronism, one of the hallmark laboratory findings is low renin levels. Renin is an enzyme secreted by the kidneys in response to low blood pressure, dehydration, or low sodium levels. When the kidneys detect these changes, they release renin, which activates the angiotensinogen-to-angiotensin pathway, ultimately stimulating aldosterone release from the adrenal glands. This process is vital for regulating blood pressure.
However, in Conn syndrome, aldosterone is produced in excess, even when the body's renin levels are low, leading to a disruption in the normal regulatory mechanisms. Low renin levels, when combined with high blood pressure, are often a red flag for primary hyperaldosteronism.
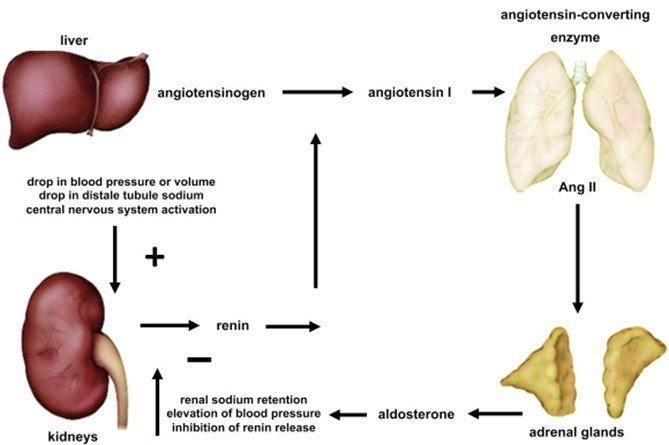
Figure 2. How aldosterone and renin control the blood pressure, sodium, and potassium in your body.
The Role of Adrenal Tumors in Conn Syndrome
Conn syndrome is often caused by benign adrenal tumors called aldosterone-producing adenomas (APA), which result in excessive aldosterone production. The tumors are typically small, and their effects may go unnoticed until the patient presents with hypertension. Adrenal hyperplasia, an enlargement of both adrenal glands, is another cause of primary hyperaldosteronism, though it is less common than aldosterone-producing adenomas.
The presence of an adrenal tumor in the context of low renin and high blood pressure can help clinicians narrow down the potential cause of hypertension. However, not all adrenal tumors result in Conn syndrome, and not all patients with primary hyperaldosteronism have detectable tumors. For this reason, screening for Conn syndrome is essential for hypertensive patients with low renin levels, especially when their blood pressure is difficult to control.
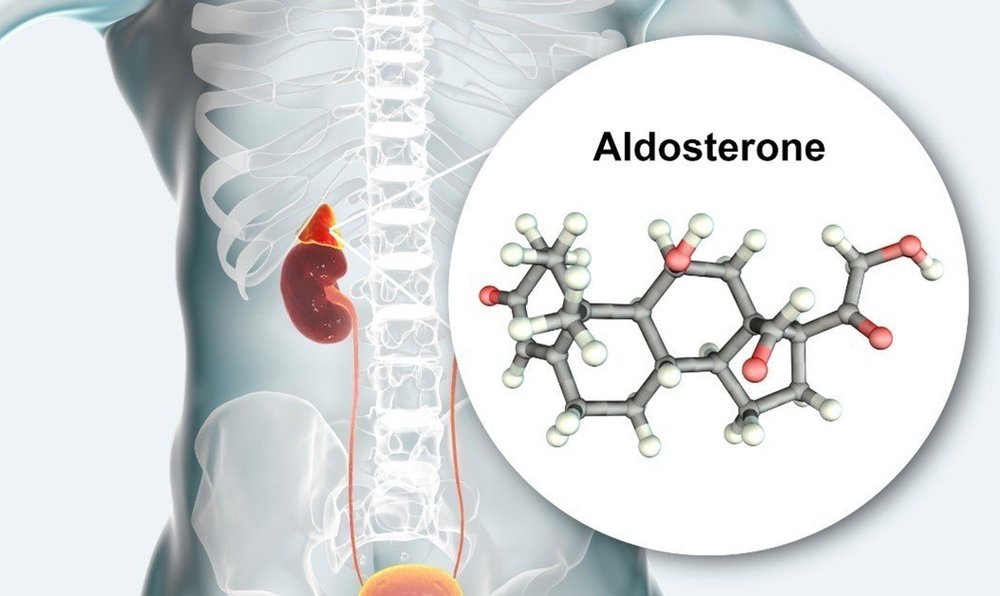
Figure 3. Too much aldosterone is very toxic for your body
Why Is It Crucial to Diagnose Conn Syndrome?
Diagnosing Conn syndrome is critical for several reasons:
1. Potential for Surgical Cure
In cases where Conn syndrome is caused by an aldosterone-producing adenoma, surgery is by far the best option. Adrenalectomy, or the removal of the affected adrenal gland, can result in a significant reduction in aldosterone levels and blood pressure normalization. For patients with unilateral aldosterone-producing adenomas, surgical removal of the tumor often provides a cure for hypertension. This is a key distinction from other forms of hypertension, which may require lifelong medication management. IMPORTANT NEWS! New data suggests that even for patients with bilateral hyperplasia (too much aldosterone from both adrenal glands) surgery (often removing one or one and a half adrenal glands) is better than medications alone.
2. Improved Blood Pressure Control
Patients with primary hyperaldosteronism often experience difficulty managing their hypertension, particularly with traditional antihypertensive medications. Conn syndrome is frequently associated with resistance to standard blood pressure drugs such as ACE inhibitors, angiotensin II receptor blockers (ARBs), or calcium channel blockers. By correctly identifying the condition and targeting the underlying cause, doctors can offer more effective treatment options, often resulting in better control of blood pressure.
3. Prevention of Long-Term Health Complications
Uncontrolled hypertension and primary hyperaldosteronism increase the risk of developing several serious health conditions, including heart disease (heart attacks, and arrhythmias; atrial fibrillation is the most common), stroke, kidney damage, and vision loss. By diagnosing Conn syndrome and addressing the underlying cause, patients reduce their long-term risk of these complications. Additionally, hypokalemia (low potassium levels), another potential consequence of primary hyperaldosteronism, can lead to muscle weakness, fatigue, and arrhythmias if left untreated.
4. Early Detection of Adrenal Tumors
While most adrenal tumors causing Conn syndrome are benign, some tumors may be malignant. Early detection and intervention can help prevent the spread of cancerous cells and improve the prognosis for affected patients. For this reason, it is crucial to rule out any malignancy when an adrenal tumor is suspected.
Who Should Be Screened for Conn Syndrome?
Not all patients with high blood pressure will have Conn syndrome. However, many do, up to 10 % of all patients with high blood pressure! Certain groups of people may be more likely to have this condition and should be considered for screening:
- Patients with Resistant Hypertension: Resistant hypertension is defined as blood pressure that remains above target despite the use of three or more antihypertensive medications, including a diuretic. If a hypertensive patient is difficult to treat, low renin levels should raise suspicion for primary hyperaldosteronism, and further diagnostic testing should be pursued.
- Patients with Low Potassium Levels: Hypokalemia (low potassium) is a common finding in patients with Conn syndrome, particularly when it is unexplained. Low potassium levels can cause muscle weakness, fatigue, and heart arrhythmias. If a patient with high blood pressure presents with hypokalemia, Conn syndrome should be considered.
- Young patients, i.e. patients with Early-Onset Hypertension: Hypertension that develops at a younger age (before 50) or with minimal family history is another red flag for secondary causes, including Conn syndrome. Such patients should undergo screening for primary hyperaldosteronism, as it may be an underlying cause of their high blood pressure.
- Patients with Unilateral Adrenal Tumors: When imaging studies (like a CT scan or MRI) reveal a unilateral adrenal mass, it raises the possibility of an aldosterone-producing adenoma, which can lead to Conn syndrome. These patients should be carefully evaluated for primary hyperaldosteronism.
How is Conn Syndrome Diagnosed?
The diagnosis of Conn syndrome involves several steps, typically starting with laboratory testing followed by imaging studies and, in some cases, specialized procedures.
- Initial Blood Tests: To screen for Conn syndrome, doctors will typically start by measuring aldosterone and renin levels in the blood. A low renin-to-aldosterone ratio (ARR) is a key indicator of primary hyperaldosteronism. If this ratio is abnormal, further diagnostic testing will be needed.
- Imaging Studies: Once Conn syndrome is suspected, imaging tests, such as a CT scan or MRI of the adrenal glands, are performed to detect any adrenal tumors or signs of adrenal hyperplasia. CT adrenal protocol is the best scan.
- Adrenal Vein Sampling (AVS): In some cases, a more invasive procedure called adrenal vein sampling (AVS) is used to determine whether one or both adrenal glands are producing excess aldosterone. This test involves sampling blood from the adrenal veins to compare aldosterone production levels from each gland, helping to determine whether the condition is unilateral or bilateral. Read more here about adrenal vein sampling: https://www.adrenal.com/blog/why-adrenal-vein-sampling-isn-t-always-necessary-with-examples
Key Takeaways
- Primary hyperaldosteronism (Conn syndrome) is a potentially reversible cause of secondary hypertension that is often overlooked.
- Hypertensive patients with low renin levels and unexplained high blood pressure should be evaluated for this condition.
- Early diagnosis and treatment can improve blood pressure control, prevent long-term health complications, and cure hypertension in many cases.
- If you or a loved one has hypertension do get screening for Conn syndrome. It is easy and inexpensive and can prevent you from stroke, heart attacks, kidney failure, and many other problems.
- Early intervention is key to managing this potentially curable cause of high blood pressure.
Dr. Tobias Carling, of the Carling Adrenal Center, is one of the world's leading experts in adrenal gland surgery. Dr. Carling performs more adrenal operations than any other surgeon in America. Dr. Carling left Yale University in 2020 to open the Carling Adrenal Center in Tampa, Florida.
To discuss the details of your case with Dr. Carling and become his patient, fill out the new patient form and he will be in touch with you shortly.
Additional Resources:
- Learn more about the Carling Adrenal Center
- Learn more about Dr. Tobias Carling
- Learn more about our sister surgeons at the Norman Parathyroid Center, and Clayman Thyroid Center.
- Learn more about the Hospital for Endocrine Surgery