4 Things to Know about Hyperaldosteronism and Hypertension

Introduction
Primary hyperaldosteronism, also known as Conn's syndrome, is a condition characterized by the overproduction of the hormone aldosterone by the adrenal glands, leading to high blood pressure and low potassium levels. While traditionally considered a somewhat rare cause of hypertension, recent studies suggest it is much more common than previously thought. Advances in medical research have significantly improved our understanding of the pathology of primary hyperaldosteronism, revealing intricate mechanisms and genetic factors that contribute to its development.
Hyperaldosteronism and Hypertension – 4 Key Things to Know
1. The Role of Aldosterone in Blood Pressure Regulation
Aldosterone is a mineralocorticoid hormone produced by the zona glomerulosa of the adrenal cortex. It plays a crucial role in regulating blood pressure by controlling sodium and potassium balance in the body. Aldosterone acts on the kidneys to promote sodium reabsorption and potassium excretion. The reabsorbed sodium draws water into the bloodstream, increasing blood volume and, consequently, blood pressure.
In primary hyperaldosteronism, the adrenal glands produce excessive aldosterone independently of the body's regulatory mechanisms. This overproduction leads to persistent sodium retention and potassium loss, resulting in hypertension and hypokalemia. Understanding the underlying causes of this dysregulation is key to unraveling the pathology of primary hyperaldosteronism.
2. Genetic Mutations and Primary Hyperaldosteronism
Dr. Carling and his team, together with scientists around the world identified several genetic mutations associated with primary hyperaldosteronism. These mutations affect various ion channels and enzymes involved in aldosterone synthesis and secretion. One of the most well-known genetic mutations is found in the KCNJ5 gene, which encodes the potassium channel Kir3.4. Mutations in KCNJ5 result in increased sodium conductance, leading to depolarization of adrenal cells and increased aldosterone production.
Other genetic mutations linked to primary hyperaldosteronism include CACNA1D, ATP1A1, and ATP2B3. These genes encode subunits of calcium channels and ATPases, which are critical for maintaining ion balance and cellular homeostasis. Mutations in these genes disrupt normal adrenal cell function, promoting aldosterone overproduction.
Understanding these genetic mutations has significant implications for diagnosing and treating primary hyperaldosteronism.
No longer do we view the cause of primary hyperaldosteronism simply as adenoma versus hyperplasia.
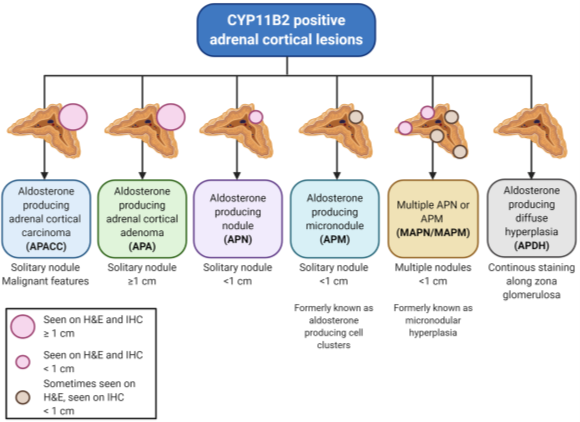
Figure 1. Classification of Aldosterone producing tumors (nodules) in Primary Hyperaldosteronism (PA). No longer do we only view them as adenoma and hyperplasia. The majority of Aldosterone producing tumors (nodules) are treated by Mini Back Scope Adrenalectomy (MBSA). From Juhlin CC, Endocrine Pathology 2021.
3. The Role of Adrenal Tumors and Hyperplasia
Primary hyperaldosteronism is often caused by either aldosterone-producing adenomas (APAs), bilateral adrenal hyperplasia (BAH) or by a combination of the two (see Figure 1). APAs are benign tumors that secrete aldosterone autonomously, while BAH involves the enlargement of both adrenal glands, leading to increased aldosterone production.
The development of APAs and BAH is influenced by genetic mutations and abnormal cellular signaling pathways. For example, somatic mutations in the KCNJ5 gene are commonly found in APAs, contributing to their autonomous aldosterone production. In BAH, genetic mutations and environmental factors may play a role in stimulating the growth and function of adrenal cells.
Advances in imaging techniques and CT scans have improved the detection and characterization of these adrenal abnormalities. This has allowed for more accurate diagnosis and targeted treatment of primary hyperaldosteronism.
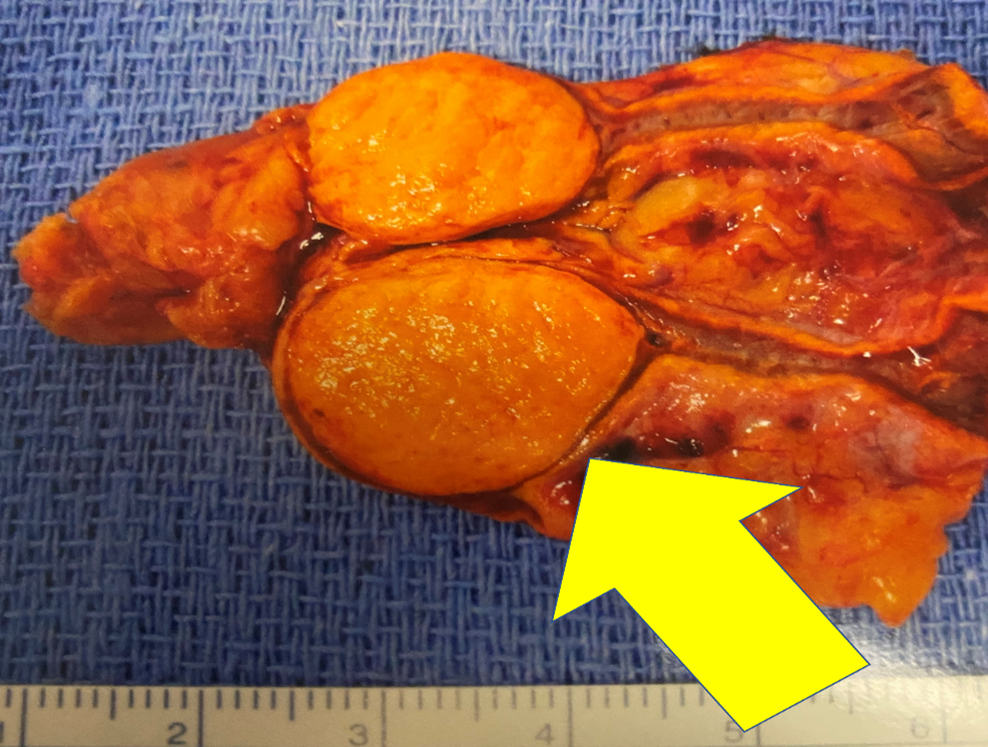
Figure 2. Typical aldosterone producing adrenal tumor causing Conn’s syndrome after it was removed.
4. Treatment: Which adrenal surgeon and operation are best?
Dr. Carling is the world’s leading expert in adrenal gland surgery and curing hyperaldosteronism. When performed by Dr. Carling, a mini back scope adrenalectomy (MBSA) for hyperaldosteronism (Conn's Syndrome) typically takes less than 20-30 minutes.
Without a doubt, the best operation for removing the adrenal tumor that is causing hyperaldosteronism and Conn's syndrome is the MBSA. The operation can also be called the Mini Posterior Retroperitoneoscopic Adrenalectomy, because the operation is performed with very small scopes that go through the lower, outer back. The Mini Back Scope Adrenalectomy (MBSA) is the preferred technique in over 95% of adrenal surgery cases, and close to 100% in patients with primary hyperaldosteronism.
Dr. Tobias Carling, of the Carling Adrenal Center, is one of the world's leading experts in adrenal gland surgery. Dr. Carling performs more adrenal operations than any other surgeon in America. Dr. Carling left Yale University in 2020 to open the Carling Adrenal Center in Tampa, Florida.
To discuss the details of your case with Dr. Carling and become his patient, fill out the new patient form and he will be in touch with you shortly.
Additional Resources:
- Learn more about the Carling Adrenal Center
- Learn more about Dr. Tobias Carling
- Learn more about our sister surgeons at the Norman Parathyroid Center, Clayman Thyroid Center and Scarless Thyroid Surgery Center
- Learn more about the Hospital for Endocrine Surgery